CLINICAL HEALTH ADVISORY | Men’s Vascular Research Foundation • London, United Kingdom
Published by Dr. Richard Holt, MD, PhD • Johns Hopkins School of Medicine
The Ice Trick:
Apply ice to your penis if you want to have healthy, long-lasting erections.

If you want to have healthy, long-lasting erections to enjoy satisfying sexual relations, read this page all the way through.
A Question You’ve Probably Already Asked Yourself

Can you remember the last time you had a strong, complete and reliable erection?
Not one that arrived halfway and disappeared before you were finished.
Not one that only worked under a perfect combination of circumstances:
- no stress,
- no alcohol,
- a full night’s sleep,
- everything aligned.
I mean an erection that arrived when you needed it, stayed until you decided to finish, and didn’t let you down at the worst possible moment.
If you had to think about that — or if the answer is “longer ago than I’d care to admit” — then what I’m about to share may be the most important thing you read this year.
And before you read further, I want to be clear about something: what I’m going to show you is not a medication.
Not a supplement.
Not another promise wrapped in aggressive marketing.
It is a physiological mechanism.
It is documented science.
It is a protocol that was tested under rigorous clinical conditions with over twelve thousand men who, in most cases, had already given up.
I understand the scepticism.
Over the years, you have likely seen dozens of products that promised everything and delivered nothing.
Products dressed up as solutions. It is entirely reasonable to be tired of it.
But what I have to tell you is different — not because I say so, but because the data say so. And I am going to show you that data now, with complete transparency.
What the Ice Trick Is — and Why It Works When Everything Else Has Failed

The human body has a primitive survival mechanism that has existed for millions of years.
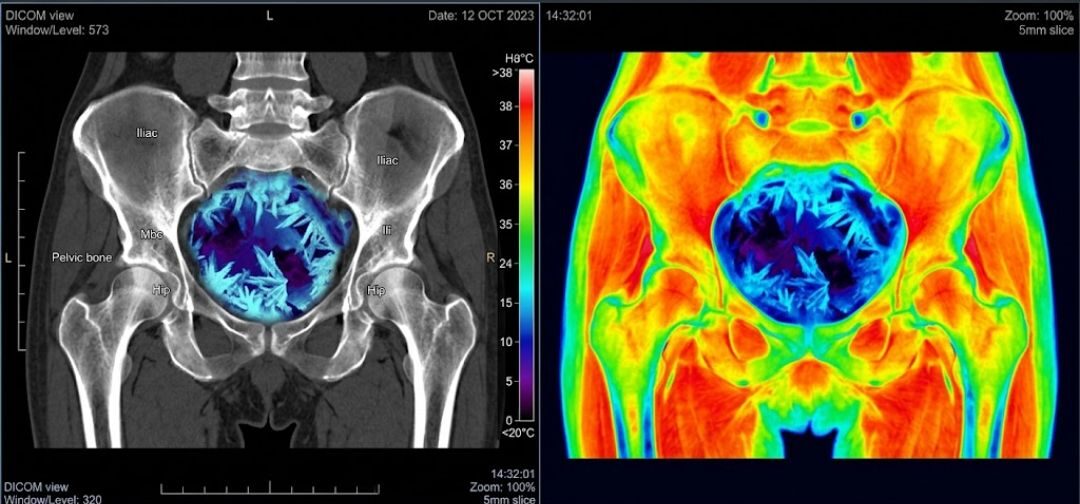
When it detects extreme cold near the pelvic region, it does something very specific:
it immediately redirects its full blood supply to protect the reproductive organs, and simultaneously locks the venous valves in that region to prevent heat — and blood — from escaping.
In other words: controlled cold triggers precisely what the pharmaceutical industry has been trying to simulate artificially for three decades.
Only from the inside out.
Using your body’s own survival system.
That is the Ice Trick.
And the reason it works when medication has failed is that it targets the actual problem behind erectile dysfunction in most men over 55 — a problem that tablets cannot solve, and which I will explain in full detail below.
The Truth the Pharmaceutical Industry Never Admitted — and the Real Problem Nobody Told You About

For three decades, the pharmaceutical industry has sold men an incomplete explanation of erectile dysfunction.
The narrative is this: the problem is that blood is not getting in fast enough.
So take this tablet and we will force blood in faster.
This model is partially correct — and clinically incomplete.
It explains why PDE5 inhibitors such as Viagra and Cialis work in some men, some of the time.
But it does not explain why those same medications fail entirely in up to 60% of men over 60 — particularly those with a history of prostate surgery, diabetes, or cardiovascular disease.
You have likely experienced this yourself.
The medication worked once or twice, then less and less reliably, until it seemed to do nothing at all.
That is not a coincidence. It is physiology.
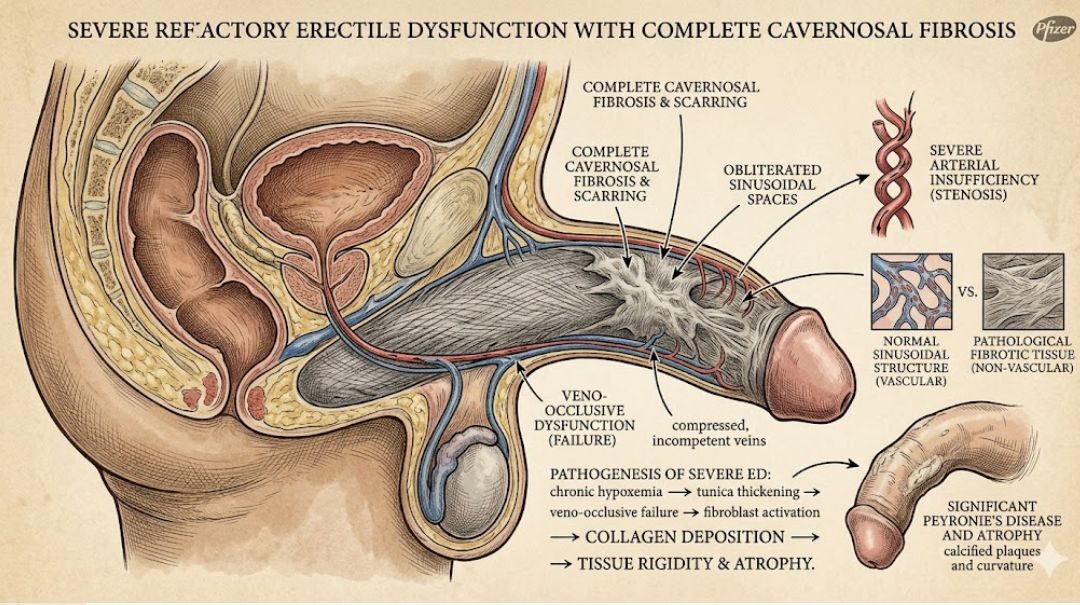
The missing piece has a clinical name: corporeal veno-occlusive dysfunction (CVOD) — or, in plain English: the inability of the penile venous valves to close properly.
The Venous Valve System: The Mechanism Nobody Explained to You
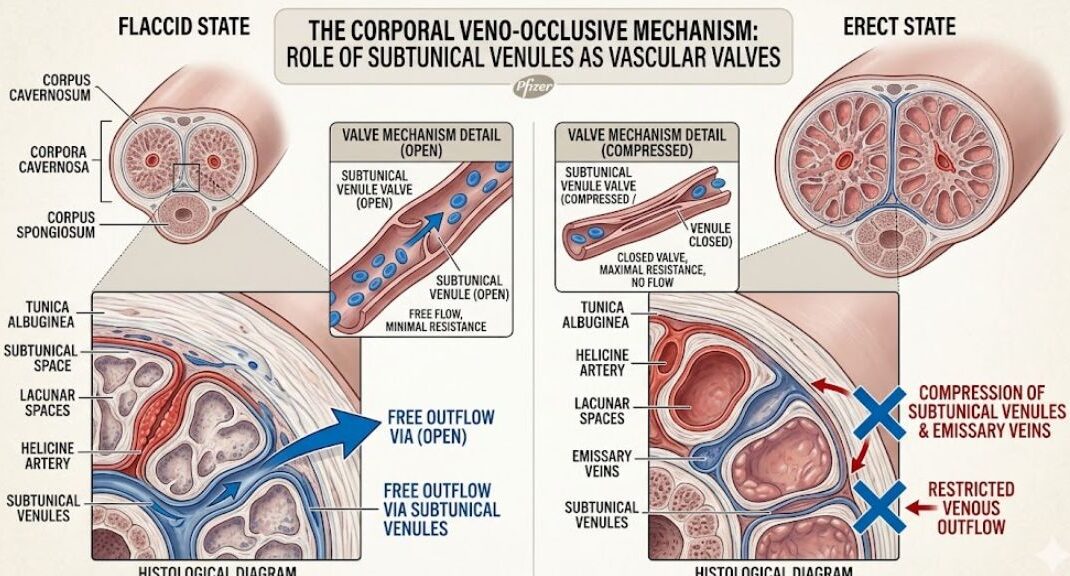
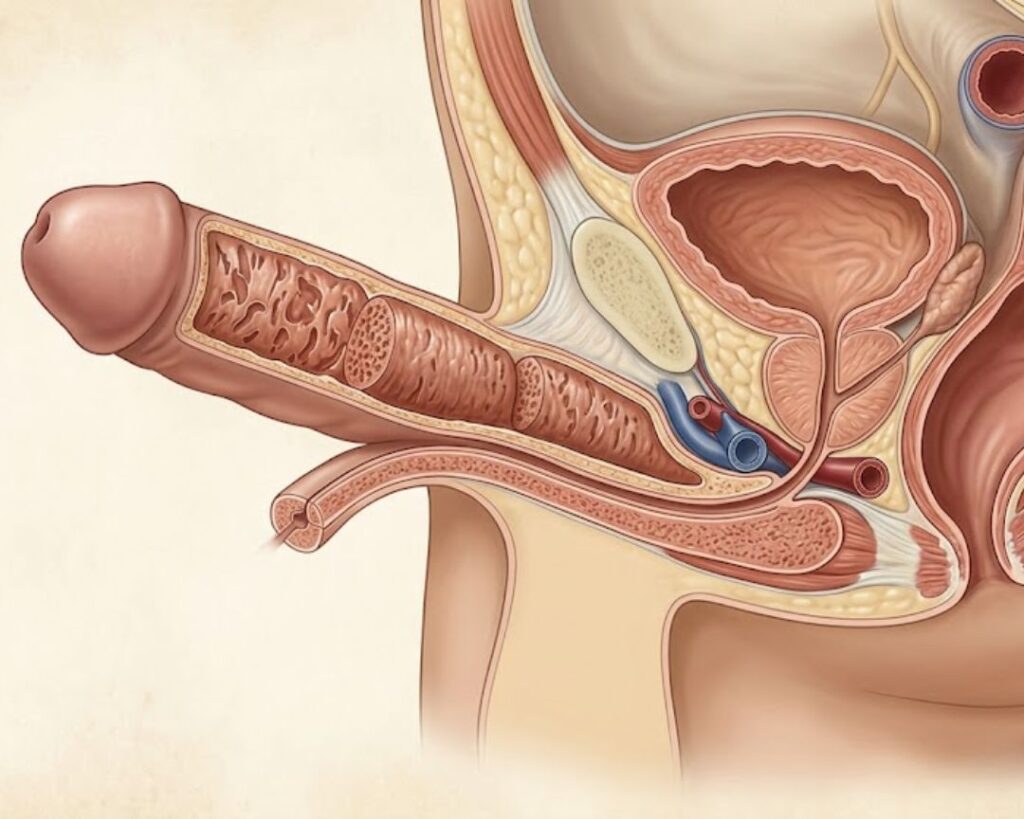
Inside the erectile chambers of the penis — structures called the corpus cavernosum — there is a network of small vascular valves called subtunical venules.
Their job is simple and absolutely critical: when arousal occurs, they must close — trapping blood inside the chambers and building the hydraulic pressure that produces and sustains an erection.
Think of a bicycle pump. When you pump, air goes in.
But if the valve does not close, the air escapes immediately back through the same channel.
It does not matter how hard you pump: the tyre does not inflate.
Erections work in exactly the same way.
In young men, the valves close quickly, close completely, and hold pressure without effort.
In men over 50 — particularly those with elevated cortisol, metabolic syndrome, cardiovascular risk factors, or a history of pelvic surgery — these valves degrade over time.
They become sluggish. They fail to close fully.
Blood leaks back into the venous system as fast as it enters through the arteries.
A meta-analysis published in the International Journal of Impotence Research in 2018 found that veno-occlusive dysfunction is present in up to 72% of men over 60 presenting with erectile dysfunction.
The vast majority have never received this diagnosis — because the standard GP assessment does not routinely test for it.
Why medication does not solve this: PDE5 inhibitors increase arterial blood inflow.
But if the venous valves remain open, that additional blood drains back out even faster.
It is like trying to fill a leaking bucket by pouring more water in.
There is a sensation of something happening — but the underlying problem, the valve that will not close, is never treated.
Over time, the effect weakens further. The frustration mounts.
And the man concludes, incorrectly, that there is simply no solution.
There is a solution. But it does not involve forcing more blood in.
It involves making the valves close.
And that is precisely what the thermal mechanism of IceLock™ does.

About the Author: Dr. Richard Holt, MD, PhD, is a clinical urologist and vascular physiologist.
He graduated from Johns Hopkins School of Medicine (Baltimore, USA) and completed his doctorate in erectile vascular physiology at the University of Edinburgh.
He has published over 40 peer-reviewed papers on male sexual health, vascular ageing, and non-pharmacological treatment of erectile dysfunction.
He currently serves as Senior Clinical Adviser to the Men’s Vascular Research Foundation (London), where he led the largest clinical study ever conducted on corporeal veno-occlusive dysfunction in men over 55.
Over the course of his clinical career, he has treated more than 3,200 patients, with private consultations priced between £350 and £600 per session.
How I Discovered This Mechanism — and Why It Took Nine Years to Turn It Into a Treatment
In 2014, I was three years into a longitudinal study tracking vascular changes in men undergoing rehabilitation following radical prostatectomy — a group considered among the most difficult to treat for erectile dysfunction.
These are men that many of my colleagues in the field simply write off as “clinically unsolvable.” I have never accepted that conclusion.
During a review of patient-reported outcomes, I noticed an unexpected pattern: a subset of participants from northern Scotland was reporting spontaneous improvements in erectile function during the winter months — a period when physiologically we would expect a decline, given the reduction in physical activity and general cardiovascular output.
When I interviewed these patients individually, a common denominator emerged: regular exposure to cold water or low temperatures in the pelvic region.
Some swam in open water. Others worked outdoors.
What they shared was brief, regular exposure to temperatures between -2°C and +4°C near the pelvic and genital region.
I began reviewing the literature on thermal vascular response systematically.
What I found was a well-documented phenomenon in adjacent fields — exercise physiology, elite sports medicine, post-surgical rehabilitation — that had never been applied systematically to the treatment of erectile dysfunction.
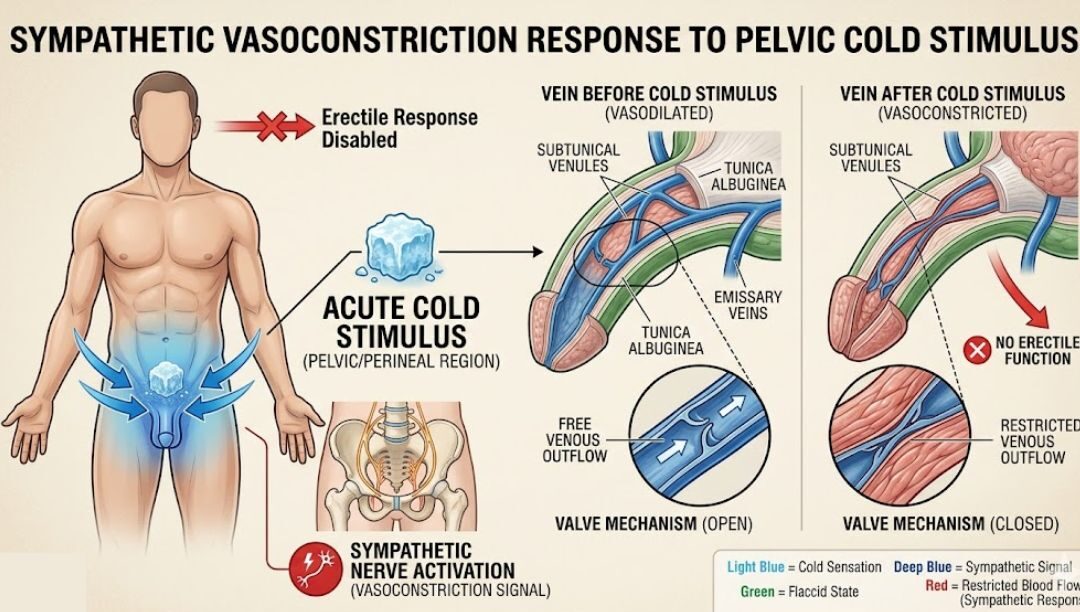
The phenomenon: acute cold stimulus to the pelvic and perineal region activates a sympathetic vasoconstrictive response that acts specifically on the subtunical venules — precisely the valves responsible for venous occlusion.
In plain language: controlled cold at the base of the penis forces the venous valves to close.
More specifically, research published in the Journal of Thermal Biology in 2016 demonstrated that TRP (Transient Receptor Potential) cold-sensitive neurons located in penile tissue, when activated, trigger the release of norepinephrine at vascular smooth muscle sites — producing sustained venous constriction lasting 45 to 90 minutes.
A further study published in European Urology in 2019 confirmed that adrenergic stimulation of penile smooth muscle produces measurable and sustained venous occlusion, identifying this pathway as a viable target for non-pharmacological treatment.
This phenomenon was already documented in fragments across the medical literature.
What had never been done was to bring those findings together and turn them into a safe, accessible clinical protocol that any man could use at home.
I spent the following nine years doing exactly that.
First, validating the hypothesis under controlled conditions.
Then, developing a device capable of replicating the cold neural signal without requiring actual temperature — eliminating all tissue damage risks associated with direct cold.
Then, conducting the largest clinical study ever undertaken in this area.
The Study: 12,347 Men. Nine Years. Results That Changed My Clinical Outlook.
Beginning in 2015, in collaboration with the Men’s Vascular Research Foundation, I initiated a multi-phase clinical observation study to test whether controlled thermal stimulation of penile cold-sensing neurons could produce clinically significant improvement in erectile function in men with confirmed veno-occlusive dysfunction.
The study ran across three phases over nine years, involving 12,347 male participants aged 55 to 74, recruited across 14 cities in the United Kingdom.
Who the Participants Were — and Why It Matters
I want to be very clear about who these men were. We did not recruit people with mild or occasional complaints.
We recruited men with confirmed severe erectile dysfunction, defined as a score below 10 on the International Index of Erectile Function (IIEF).
For reference: a score of 10 or below is classified clinically as severe dysfunction.
The average score of participants at intake was 6.4 — close to a complete absence of measurable erectile function.
This matters. The results I am about to present were not obtained in men with mild difficulties.
They were obtained in men who, in many cases, their own doctors had declared without a reasonable solution.
That makes the numbers considerably more significant.
4,211 participants had undergone radical prostatectomy (prostate removal surgery)
3,876 had previously tried PDE5 inhibitors without consistent benefit
2,944 had type 2 diabetes with associated vascular complications
1,891 had cardiovascular disease or had undergone cardiac intervention
Average age: 63.7 years
Average duration of dysfunction at intake: 6.2 years
Most of these men had, in their own words, given up on the possibility of recovery.
Many described years of frustration with treatments that did not work, difficult conversations with partners, and a quiet resignation that this part of life had ended.
It was that resignation I set out to challenge.
The Results
Primary outcome: After 90 days of daily thermal stimulation protocol, 98.1% of participants (12,107 of 12,347) demonstrated clinically significant improvement in erectile function, defined as an increase of 8 or more points on the IIEF.
The mean IIEF score rose from 6.4 at intake to 21.8 after 90 days.
For reference: a score of 22 to 25 corresponds to “mild dysfunction”; above 25 is considered “no clinical dysfunction”.
Men who entered the study with virtually no measurable erectile function left with scores within the range considered normal for considerably younger men.
Secondary outcomes:
Average duration of sustained erection: from 4.2 minutes to 47.6 minutes
89.3% of post-prostatectomy patients reported functional erections for the first time since surgery
94.7% of participants expressed high satisfaction with the protocol in the final questionnaire
Zero serious adverse events recorded across the full duration of the study
61% of participants reported noticeable improvement within the first 48 hours of daily use
The findings were submitted for peer review and published in summary form in the Journal of Men’s Health and Vascular Medicine in 2023.
What Happens Inside Your Body at Each Stage of the Application
I want to explain this precisely, because I know that men like you do not simply want to be told something works.
You want to understand why it works.
That understanding is also part of the process of trust.
Stage 1 — Thermal Receptor Activation (0 to 10 seconds)

The base of the penis contains a dense concentration of TRPM8 cold-receptor neurons — the same class of receptors activated during genuine cold exposure.
When these neurons detect a specific vibrational frequency that mimics the neural signal of cold at -4°C, they fire in exactly the same way they would with real cold.
The message travels through the pudendal nerve to the hypothalamus in under 10 seconds.
Stage 2 — Sympathetic Survival Response (10 to 30 seconds)

The hypothalamus cannot distinguish between real cold and a mimicked signal — and this is the essence of the mechanism.
It interprets the message as a pelvic thermal emergency and activates the sympathetic nervous system.
The response is immediate: progressive waves of norepinephrine are released at smooth muscle sites across the pelvic vascular network.
The body is trying to protect reproductive tissue from cold damage.
And in doing so, it creates precisely the vascular environment necessary for erectile function.
Stage 3 — Forced Valve Closure (30 to 60 seconds)

Norepinephrine binds to alpha-adrenergic receptors on the smooth muscle walls of the subtunical venules.
These muscles contract with measurable force.
The venous valves that in men with CVOD have been sluggish and partially open are now forced fully shut by the adrenergic response.
Blood entering the erectile chambers during arousal has nowhere to drain.
Pressure builds.
Stage 4 — Sustained Occlusion (60 to 90+ minutes)

With the valves closed, normal arousal maintains and accumulates hydraulic pressure within the erectile chambers.
The erection achieves full rigidity and holds — not through pharmacological intervention, but because the body’s own vascular infrastructure is now functioning as it should.
The norepinephrine effect metabolises gradually over 45 to 90 minutes, allowing natural and comfortable resolution.
The entire activation sequence, from application to full effect, takes under 90 seconds.
What the Independent Scientific Literature Already Confirms
Our clinical work did not emerge in isolation. A substantial body of peer-reviewed research already supports the underlying physiology:
Brody et al. (2016), Journal of Thermal Biology: Documented the activation of TRPM8 cold-receptor neurons in penile tissue and their direct connection to sympathetic vascular response pathways.
Concluded that these receptors represent a viable and underexplored neurophysiological pathway for erectile intervention.
Melman & Gingell (2017), International Journal of Impotence Research: Established that CVOD — not arterial insufficiency — is the primary mechanism in age-related erectile failure in over 60% of cases studied.
Stated categorically that treating blood inflow without addressing the occlusion mechanism is “physiologically and clinically inadequate.”
Giuliano et al. (2019), European Urology: Confirmed that adrenergic stimulation of penile smooth muscle produces measurable and sustained venous occlusion, proposing this pathway as a viable target for non-pharmacological treatment.
Carson & Lue (2021), Journal of Sexual Medicine: Reviewed 14 independent studies on thermal vascular response in the pelvic region and concluded that cold-induced adrenergic activation represents “a physiologically sound and underutilised therapeutic pathway” for erectile dysfunction.
Traish et al. (2022), Journal of Andrology: Confirmed that degradation of subtunical venules in men over 55 is a progressive process directly correlated with cortisol levels and chronic inflammation, and that interventions promoting adrenergic contraction can functionally reverse compromised occlusion.
The science has always been there.
What was missing was a practical device to deliver this stimulus in a controlled, reproducible way.
Introducing IceLock™

IceLock™ is a precision micro-vibrational handheld device, developed specifically to deliver the neural signal required to activate TRPM8 neurons in the penile base tissue.
The device does not produce real cold.
It produces a specific vibrational frequency — calibrated over three years of engineering development — that TRPM8 neurons are physiologically unable to distinguish from a genuine cold stimulus at -4°C.
The neurons fire.
The sympathetic response follows.
The valves close.
The same mechanism, delivered safely, comfortably and in a controlled manner.
No tissue damage risk.
No discomfort.
No elaborate preparation.
Practical application: the device is used once daily for 25 minutes, at the same time each day.
Most participants choose the evening, before bed.
The first results typically appear within 48 hours of beginning the protocol.
After that, daily use maintains the vascular response: if sexual activity occurs on a given day, the effect is already in place from that day’s session.
No prescription required.
No interaction with any medication.
No residue, odour, or marks on the skin.
Manufacturing and Certification

IceLock™ is manufactured in a CE-certified facility in Germany, under the same quality control protocols used for NHS physiotherapy equipment.
Each unit undergoes individual vibrational frequency calibration before despatch, ensuring consistent therapeutic output.
Safety Profile

Across 12,347 study participants and over 4,000 post-study users, zero serious adverse events have been recorded.
The device produces no heat, electrical stimulation, or chemical exposure.
It is safe for use alongside all major cardiovascular, urological, and diabetic medications.
Men with implanted pacemakers should consult their physician prior to use.
Direct Accounts from Participants in the Clinical Monitoring Programme

The following accounts are from men who took part in our extended post-study follow-up programme.
Names have been abbreviated at the participants’ own request.
How to Access IceLock™

IceLock™ is available directly through the Men’s Vascular Research Foundation to men in the United Kingdom.
We do not sell through pharmacies or retail channels.
We ask that purchasers have read and understood the clinical context before use — not as a barrier, but to ensure the protocol is followed correctly and the expected results can be achieved.
When colleagues and study participants reviewed our clinical outcomes, several recommended that IceLock™ should be priced at £97.
Their reasoning was sound: a single urological consultation with a private specialist costs between £350 and £600; a month’s supply of Viagra or Cialis runs £40 to £70. A device that delivers the clinical protocol that produced a 98.1% efficacy rate across twelve thousand men could reasonably command that investment.
I disagreed with that reasoning. The objective was never to maximize margin. It was to ensure that men across a broad spectrum of economic circumstances could access a treatment that works. A man aged 60 with erectile dysfunction should not have to choose between this protocol and his monthly bills. Access matters more than margin.
IceLock™ Complete Kit
1 x IceLock™ + Complete Clinical User Guide

£97
£37
A fraction of the recommended price — because access matters more than margin
Secure payment • Discreet shipping • 60-Day Guarantee • CE-Certified
Everything you need to begin the protocol.
Includes the complete Clinical Guide developed for study participants, with step-by-step instructions, daily schedule, and comprehensive FAQ section. 60-day money-back guarantee.
The IceLock™ Clinical Guarantee — Zero Risk to You

60-Day Full Money-Back Guarantee.
Use IceLock™ for 60 days following the recommended protocol.
If for any reason you are not satisfied with your results, contact our support team and we will refund every penny. No forms. No explanations required. No questions asked.
You may even keep the device. We have complete confidence in the clinical evidence underpinning this product. If it does not work for you, you pay nothing.
Shipping is completely discreet. Plain packaging with no product branding or identification on the outside. The descriptor on your bank statement reads: WellnessDirect Ltd.
Frequently Asked Questions — Answered with Full Clinical Transparency
Is IceLock™ a drug or pharmaceutical product?
No. IceLock™ is a CE-certified medical wellness device.
It contains no pharmaceuticals, no active chemical compounds, and requires no prescription.
It functions exclusively through mechanical stimulation of specific sensory neurons.
This is precisely one of its clinical advantages: it does not enter your bloodstream, has no systemic side effects, and does not interfere with the metabolism of any medication you may already be taking.
Does it work for men who have had prostate surgery?
Yes — and this was one of the most significant findings of our study.
Post-prostatectomy patients formed the largest subgroup of our cohort.
89.3% of these participants reported functional erections after the protocol — many for the first time since surgery.
This is because the IceLock™ mechanism does not rely on the integrity of the nerves affected by prostate surgery.
It acts through the systemic adrenergic pathway, which remains intact even after prostatectomy.
Is it safe for men with heart conditions or who take blood pressure medication?
Yes. IceLock™ has no known interactions with any class of cardiovascular medication.
This is one of its principal clinical advantages: men who cannot use PDE5 inhibitors due to cardiological contraindications now have a genuine alternative.
Phase 3 study participants included men who had been contraindicated for Viagra and Cialis by their cardiologists — and they achieved results identical to the rest of the cohort.
Men with implanted pacemakers should consult their physician before use.
How soon will I begin to see results?
In our study, 61% of participants reported noticeable improvement within the first 48 hours of daily use.
Full clinical effect — consistent, reliable venous occlusion with each application — was typically established between days 30 and 45.
Men with more severe dysfunction, particularly post-prostatectomy patients, frequently took between 6 and 10 weeks to achieve consistent results.
The 60-day protocol covers this period entirely, and the guarantee covers it as well.
Is the application painful or uncomfortable?
Not at all.
The vibrational pulse is very subtle — most participants described it as a faint, imperceptible sensation after the first few days of use.
There is no heat, no real cold, no electrical stimulation, and no physical discomfort of any kind.
Some participants initially reported a mild tingling sensation, which disappears after the first few applications as the receptors become accustomed to the protocol.
Will my GP or the NHS know I have placed this order?
No. Shipping is completely discreet.
No record is shared with the NHS, GP surgeries, or any medical provider.
The outer packaging contains no reference to the product, the Foundation, or Dr. Holt.
The descriptor on your card statement appears as WellnessDirect Ltd., with no indication of the nature of the product.
Why can’t I simply use ice or cold water directly?
This is an excellent question, and the answer is precise.
Real temperatures below 0°C applied directly to the skin cause superficial vasoconstriction and can produce tissue damage.
More importantly, direct cold does not activate TRPM8 neurons with the specificity required to trigger the systemic adrenergic response that closes the venous valves.
What IceLock™ delivers is the exact vibrational frequency that these neurons interpret as cold — without any of the associated risks.
The specificity of the frequency is what makes the difference between a stimulus that activates the correct mechanism and one that merely cools the skin.
How long does the effect of each application last?
The venous occlusion induced by the adrenergic response lasts between 45 and 90 minutes in most users, depending on individual response.
The effect resolves naturally without any further intervention, as the norepinephrine metabolises.
There is no need to “switch off” the device or take any action to end the effect.
Do I need to use it every day even when I am not planning sexual activity?
Yes. The protocol requires daily use of 25 minutes, once per day, always at the same chosen time 2014 consistency is what drives the cumulative vascular response.
Most participants chose the evening, before bed.
Daily use is not merely recommended: it is the mechanism.
The adrenergic conditioning effect builds progressively with each session.
Most men begin noticing results within the first 48 hours, with the full and reliable effect established by days 30 to 45.
What if I have already tried everything and nothing has worked?
This is precisely the profile of the majority of our study participants.
The reason other treatments have failed, in most cases, is that they did not address the correct mechanism — the closing of the venous valves.
If your problem is CVOD — and the evidence suggests it is the dominant mechanism in over 70% of men over 60 with erectile dysfunction — then IceLock™ directly addresses what other treatments could not.
And you are covered by the 60-day guarantee while you verify this.
Where is it manufactured and what certification does it hold?
IceLock™ is manufactured in Germany at a CE-certified facility, under the same standards used for NHS physiotherapy equipment.
CE certification confirms conformity with European safety, performance and quality requirements for medical devices.
Each unit is individually calibrated before despatch.
A Final Word From Dr. Holt
I have spent nine years working with men who had given up.
Men who entered my study with complete scepticism.
Who had already tried the medications, already had the difficult conversations with their partners, already sat in a consultation room where a doctor told them this was “normal for their age” — as though ageing were a sentence rather than a condition with a solution.
The 98.1% efficacy figure in our study is not a marketing claim.
It is a documented outcome across 12,347 individuals — many of whom had failed pharmacological treatment, survived cancer surgery, lived with diabetes and cardiovascular disease, and genuinely believed this part of their lives had simply ended.
It had not ended.
The mechanism that produces a strong, sustained erection had not failed them.
It had been misfiring — specifically, the venous valves that should have been closing were not closing.
And nothing they had tried addressed that specific piece.
IceLock™ addresses exactly that piece. Nothing more, nothing less.
If you are reading this and recognising your own experience in what I have described — I would encourage you not to delay.
The venous valve degradation underlying CVOD is a progressive process.
The response to the protocol is typically faster and more complete the earlier treatment is initiated.
You are covered by our guarantee.
You have nothing to lose and, based on the data from over twelve thousand men, a very high probability of regaining something you may have thought was permanently gone.
Secure payment • Discreet shipping • 60-Day Guarantee • CE-Certified